Hip Injuries
Disc Herniations
(wikipedia)
A Spinal disc herniation (prolapsus disci intervertebralis) is a medical condition affecting the spine due to trauma, lifting injuries, or idiopathic (unknown) causes, in which a tear in the outer, fibrous ring (annulus fibrosus) of an intervertebral disc (discus intervertebralis) allows the soft, central portion (nucleus pulposus) to bulge out beyond the damaged outer rings. Tears are almost always postero-lateral in nature owing to the presence of the posterior longitudinal ligament in the spinal canal.[1] This tear in the disc ring may result in the release of inflammatory chemical mediators which may directly cause severe pain, even in the absence of nerve root compression.
Disc herniations are normally a further development of a previously existing disc “protrusion”, a condition in which the outermost layers of the annulus fibrosus are still intact, but can bulge when the disc is under pressure. In contrast to a herniation, none of the nucleus pulposus escapes beyond the outer layers.
Causes & Treatment
Many disc herniations are due to one time trauma(car accident, lifting heavy objects), or cumulative trauma disorder or degeneration.
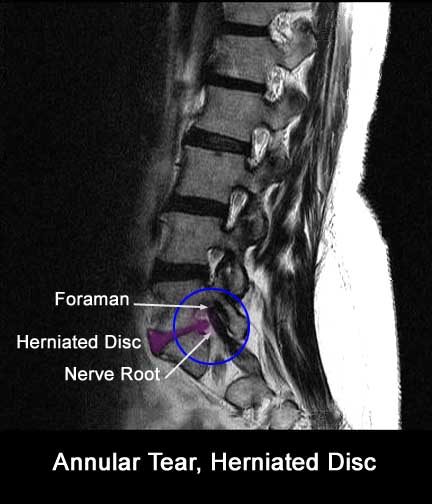
According to Dean Moyer, “To get the full story we have to go back about ten years to a study published in the New England Journal of Medicine involving the use of Magnetic Resonance Imaging (MRI) to diagnose back pain. In this study researchers (who were intrigued by the findings of several other studies concerning herniated discs) selected 98 subjects who did not have back pain or any other back related symptoms and sentthem to be evaluated by MRI scans. What makes this interesting is that the evaluators were not told that these people did not have back problems.
The results were pretty astounding and sent a shock wave through the medical community at that time. What they found was that 64 percent of the test subjects came back with MRIs that showed disc problems that normally would have marked them as prime candidates for surgery… except, of course, for one little problem… and that was that they did not have back problems at all!
Over half of the test subjects turned out to have herniated discs, and a large percentage of these people – who did not have any back pain whatsoever – were diagnosed as having such things as spondylolysis, spondylolisthesis and stenosis of the spinal canal. Here are the exact findings:
The most common nonintervertebral disk abnormalities in people without symptoms were Schmorl’s nodes (herniation of the disk into the vertebral-body end plate), in 19 percent of the subjects; annular defects (disruption of the outer fibrous ring of the disk), in 14 percent; and facet arthropathy (degenerative disease of the posterior articular processes of the vertebrae), in 8 percent. Seven percent of the asymptomatic subjects had spondylolysis, 7 percent had spondylolisthesis, 7 percent had stenosis of the central canal, and 7 percent had stenosis of the neural foramen. [1]
With the results of the two readings averaged, 52 percent of the subjects had a bulge at at least one level, 27 percent had a protrusion, and 1 percent had an extrusion. Thirty- eight percent had an abnormality of more than one intervertebral disk. [1]”
Bibliography 1. Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, et al: Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med. 1994;331(2):69-73.
Treatments
We work to treat disc herniation patients with Active Release Techniques, spinal decompression therapy, sometimes spinal manipulation.
We get results where others fail by working on any and all peripheral nerve entrapments of any affected nerves in the upper or lower extremity. This gets fast results in patients when the disc herniation is not the cause of their pain, but rather it is due to peripheral entrapment of the nerve, and the disc herniation is an incidental finding on the MRI.
Related Articles:
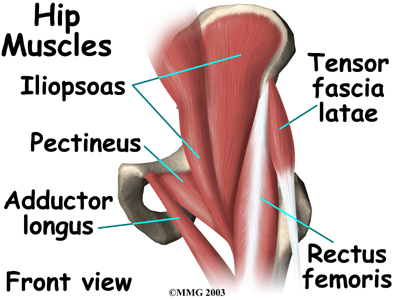
Hip Flexor Strain
A hip flexor strain is a tear in the muscles or tendons of the hip flexors, which are located in the front of the thigh where the hip and thigh meet.
Iliotibial Band Syndrome ITBS
(wikipedia)
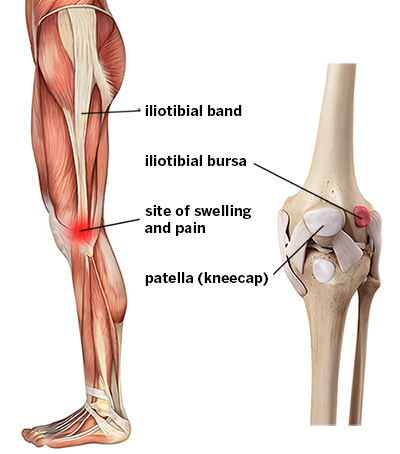
Iliotibial band syndrome is one of the leading causes of lateral knee pain in runners. The iliotibial band is a thick band of fascia on the outside of the knee, extending from the outside of the pelvis, over the hip and knee, and inserting just below the knee. The band is crucial to stabilizing the knee during running, as it moves from behind the femur to the front of the femur during activity. The continual rubbing of the band over the lateral femoral epicondyle, combined with the repeated flexion and extension of the knee during running may cause the area to become inflamed.
Causes & Treatment
ITBS is typically an overuse injury, or it can be caused by trauma. Our office treats ITBS by eliminating adhesions and fibrosis of the ITB and the quadraceps in the front of the ITB and the hamstring in the back of the ITB. Also there are commonly adhesions below the patella, where the ITB inserts onto the tibia. We use Active Release Techniques, Graston, stretching, and ultimately a strength and stabilization program to rehab the hip, knee, and lateral as well as pelvic stabilizers.
Related Articles:

Labral Tears
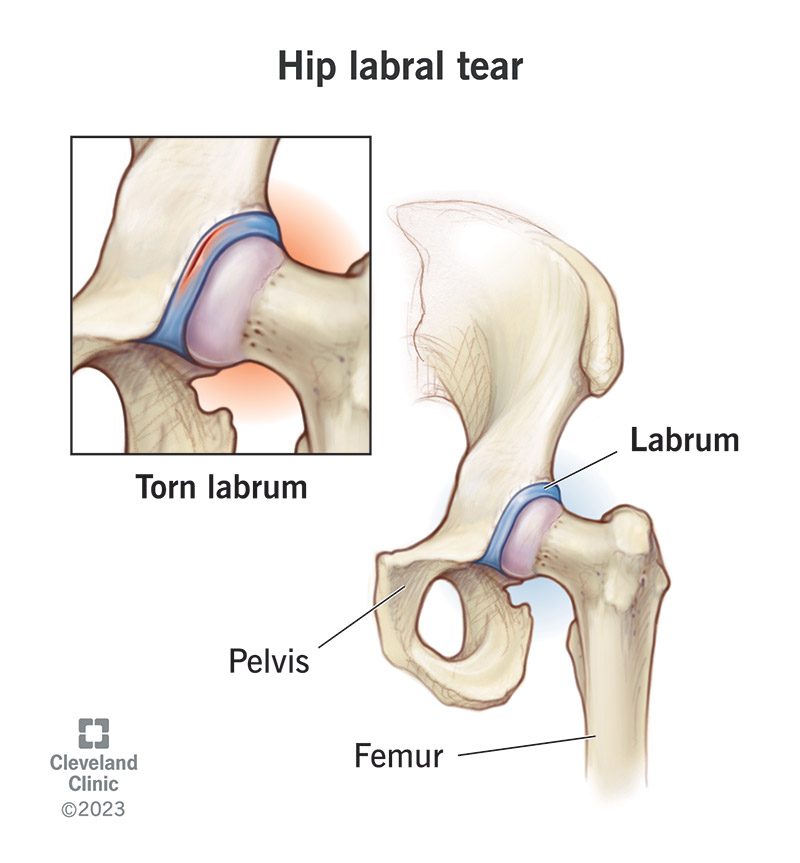
Labral tears have been a diagnosis of increasing popularity in recent years. Primarily because there is a very sensitive test for detecting the tears, and a recent procedure to repair the tears. It is debatable how many of these injuries are an incidental finding on a new sensitive test, and how many are truly the source of an athletes pain and dysfunction.
Causes & Treatment
Most labral tears are caused by trauma or cumulative trauma disorder (overuse), some are caused by rotation of the femur with a planted foot, and others by a congenital deformity of the femoral head and FAI syndrome.
Our office works to reduce any adhesions present between the psoas muscle and the labrum, as well as the surrounding anatomy. We do this Active Release Techniques, stretching, and ultimately strength and stabilization of the surrounding anatomy.
Related Articles: